Download and Read the full Covid Report by Nelle Maxey HERE (pdf)
Download and Read the Covid Report Appendix A & B HERE (pdf)
The Covid Report has two distinct sections and two appendices with more details.
Part I is a discussion of how data is being defined and propagated and why the numbers are thus seriously inflated. Part II presents Canadian and global data in different formats and analyzes what we are being shown and what we should be shown.
Appendix A: Testing contains references to many different published studies, interviews and articles and delves deeply in the problems with RT-PCR testing. It questions why Canada is not Antibody testing instead and presents data from antibody testing in other countries.
Appendix B: WHO delves into what WHO definitions are actually saying and why the members of medical professions have concerns with new, cause-of-death definitions. It also challenges WHO discussion of the similarities and differences.
“Of all tyrannies, a tyranny sincerely exercised for the good of its victims may be the most oppressive…This very kindness stings with intolerable insult. To be “cured” against one’s will and cured of states which we may not regard as disease is to be put on a level of those who have not yet reached the age of reason or those who never will; to be classed with infants, imbeciles, and domestic animals.”
– C.S. Lewis, God in the Dock: Essays on Theology
Published Posthumously, 1974
Part 1 Summary
Statistics are math, not science. Statistics do not prove anything, though they can point the way for scientific investigation and proof.
Language is powerful and definitions establish understanding. Changing long-established definitions and procedures has resulted in much confusion about what is happening with Covid-19 in global populations.
PCR testing is the basis for all Covid-19 infection data. It inflates case numbers. PRC testing is not Fit for Purpose. It does not test for the actual SARS CoV-2 virus. It has a high false discovery rate and a specificity rate of only 80–85%. The testing threshold (Ct number) is arbitrary. Antibody testing should be used now to estimate actual total case numbers.
WHO definitions also inflate case numbers as they allow “virus not present” cases to be counted as covid cases. The definitions also inflate death numbers as cause-of-death standards are changed to include anyone even suspected of having Covid-19. WHO case definitions are adopted by nations around the world, including Canada.
Transmissibility of Sars-CoV-2 virus is determined by the basic reproduction (R0) number in the beginning of an epidemic and the effective reproduction (R or Rt) number thereafter. These statistical constructs are based on assumptions fed into equations.
Severity of Sars-CoV-2 virus is estimated by Case Fatality rates (CFR) and infection fatality rates (IFR). CFRs are inflated by inflated number of deaths (numerator) and by inflated number of cases (denominator). IFRs cannot be established until the total number of cases, both symptomatic and asymptomatic, in the entire population (not just the tested symptomatic population) can be estimated. Antibody testing can be used to estimate the size of the immune population which reflects the previously infected population. Only then can a true IFR be established.
Prevalence of Covid-19 in the entire Canadian population is very low—currently at 0.2%. Extreme social controls should never be used in low prevalence epidemics.
As presented by the Public health Agency of Canada (PHAC), the modelling techniques used to establish probabilities of the epidemic trends and thus “inform” policy decisions have no basis in evidence, are completely inflated, and essentially amount to statistical chicanery.
Canada’s choice to institute early social controls will prolong the epidemic (possibly increase deaths) and guarantee successive waves of infection as social controls are lifted and susceptible individuals, previously cocooned from infection by social controls, are exposed. Opening schools offers some mitigation to waves of infection as this increases the immune population. The most fragile susceptible population must be protected, not discarded/sacrificed as has been seen to happen.
Case numbers, death numbers, transmissibility and severity of the SARS CoV-2 virus should be re-examined based on current data.
Mitigation would have been a far better strategy than suppression to protect the public’s health at the same time as not destroying their lives and livelihoods and increasing the national debt levels.
The public health concept and now politicized meme of “lockdown until a vaccine can be developed” to supposedly protect the public from a contrived epidemic is not palatable to the many, only to the few who stand to gain.
Part II DATA
Summary
Using total cases numbers as though they represented the risk of being infected with Covid-19 is perception management. While these cumulative numbers may be of interest for epidemiological study at an academic or public health level, they have little bearing on the true situation facing citizens.
Active case numbers plus recovered case numbers and associated deaths should be the presentation style chosen for public consumption. Prevalence and Risk should be discussed instead of inflaming public fear.
Rather than chanting “there is no cure”, public health officials should offer positive, mitigation of risk advice, including the importance of good nutrition and daily Vitamin C and D supplementation during epidemics.
Many scientists and doctors have expressed confidence in high dose IV vitamin C, vitamin D supplementation and other generic, inexpensive and readily available medications to assist recovery. It is simply not true there is no cure.
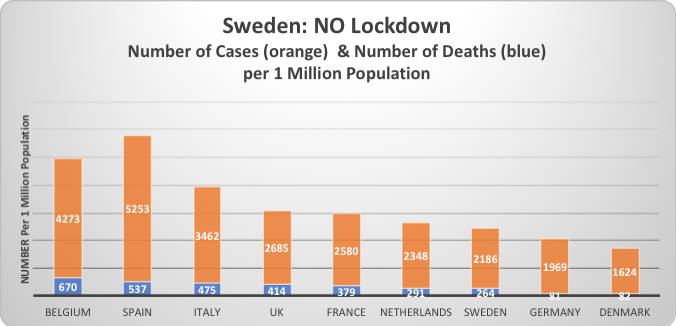
This chart is based on WorldOmeter data published on May 2, 2020