Home Risk of Death from Non-vaccination Compared to Vaccination
Vaccines are universally promoted as “safe and effective” regardless of the vaccine, ingredients, mode of action, or recipient age. To validate the claim of “safe and effective”, every vaccine ought to be evaluated for both efficacy and safety.
The fact that, in the US, hundreds of thousands of adverse effects and deaths have been reported to Vaccine Adverse Events Reporting System (VAERS) despite only few doctors being even aware of VAERS’ existence, and that of those, over a thousand compensation claims are paid each year despite the highly restrictive legal obstacles that have been artificially imposed to any successful claim, would seem to challenge the claim of “safety”. A more robust analysis of safety is needed to assist parents and other adults to make an informed decision.
Ultimately the question to be addressed is –
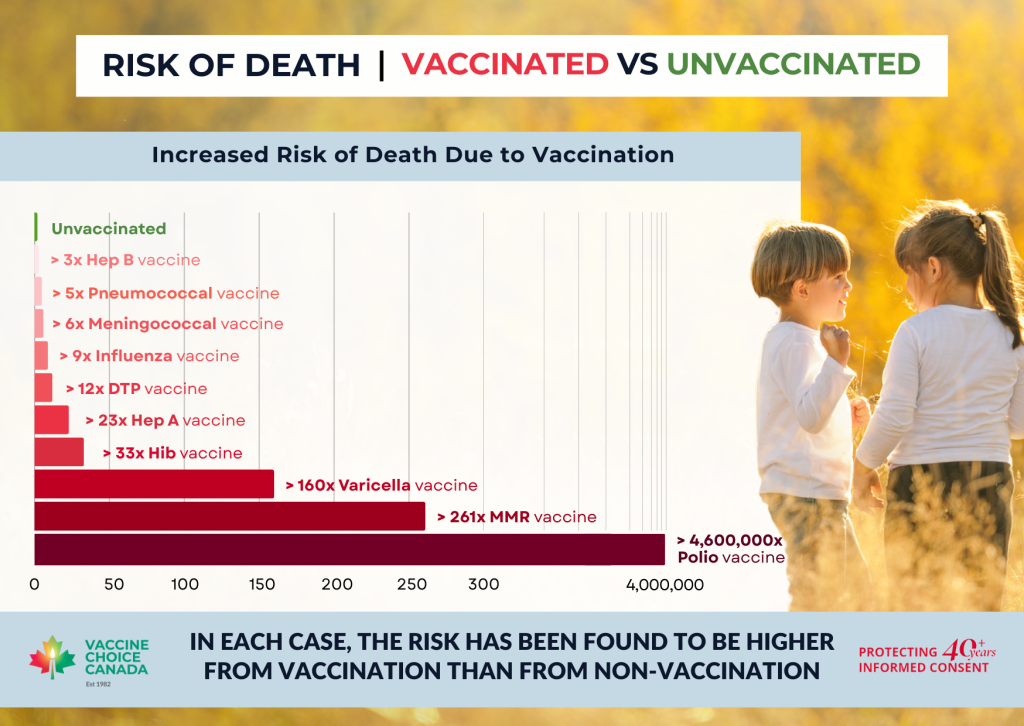
Is the increased risk of dying from an illness or suffering a serious adverse condition from being unvaccinated less or greater than the risk of such from being vaccinated?
To enable an informed decision, information quantitatively determined and provided to the decision-maker ought to include:
Incredibly, no government agency has conducted any such comprehensive, quantitative analysis and thus proven that any vaccine is of overall benefit. Instead, a vaccine’s overall benefit is “assumed”, often based primarily on its ability to induce the production of antibodies, without giving due consideration to known or possible serious risks, which are dismissed nonchalantly with unsubstantiated claims that injuries are “rare”.
A mathematician has noted the lack of proper mathematical demonstration in medical literature that the risk of a serious adverse effect or death from illness as a result of not vaccinating is higher than that from vaccinating. Hence, the mathematician has conducted a thorough comparison of those risks, mathematically incorporating all critically relevant data to the extent that is reasonably possible.
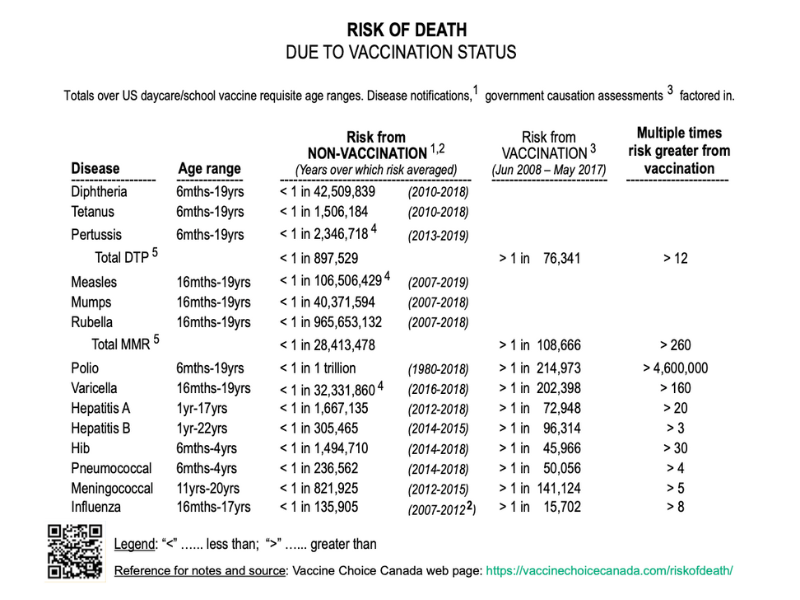
The comparative analysis covers each vaccine mandated in the US for enrolment of under 20 year olds in childcare or educational institutions, and relies upon recent historical data and research findings that are collected or respected by government.
The details and results of that analysis are in a Judicial Notice (a legal document) entitled “Numerical risk comparison of non-vaccination versus vaccination”, located here: https://vaxcheckers.org/wp-content/uploads/2021/09/PRJN4.pdf
For further information, see this published peer-reviewed paper: ‘Health versus Disorder, Disease, and Death: Unvaccinated Persons Are Incommensurably Healthier than Vaccinated’ https://ijvtpr.com/index.php/IJVTPR/article/view/40
The findings of that analysis were that in the case of both death and suffering a serious adverse condition, the risk is higher from being vaccinated than from being unvaccinated.
These results alone should cause every adult and parent to pause.
Reference Notes
1. Importantly, the chance of an unvaccinated person contracting a vaccine-targeted disease falls far short of 100%, e.g. average annual tetanus notifications in the US totaled only approximately 3.5 across the relevant age range. Based upon an average vaccination coverage of 95% and claimed effectiveness (incorporating waning) of 92%, the average annual tetanus incidence in the totally unvaccinated in this age range still works out at approximately 1 in 3,000,000. Note also that tetanus is not contagious, so none of the protection enjoyed by the unvaccinated is attributable to vaccination of any contact(s).
2. This level of risk is the incremental risk of death from the vaccine-targeted disease for an unvaccinated person above that for a vaccinated person. It is based upon the result of combining government records of disease notifications and vaccine coverages and government claims of vaccination effectiveness, and an assumption that observed, interpolated and extrapolated vaccine-induced antibody levels pre- and post- waning can be taken to equal the respective vaccine effectiveness levels that remain at those times. The risk is calculated for each age group within the applicable age range using the following formula, and then totaled across those age groups:
SRIUD = SRPD x VE / (1 – (VC x VE)), where:
SRIUD is the risk of death attributable to not being vaccinated,
SRPD is the rate of deaths attributed or attributable to the disease,
VE is the government-claimed vaccination effectiveness (incorporating antibody waning rate), and
VC is the vaccination coverage.
3. This risk incorporates the estimate published in “Electronic Support for Public Health – Vaccine Adverse Event Reporting System (ESP:VAERS)” (2011, HHS grant) that <1% of serious adverse events (SAE) post-vaccination are reported to VAERS, but also incorporates vaccine SAE causation assessments made or respected by government. “Probable” causation is assumed to be “certain” whereas “possible” causation is disregarded. Attribution of causation is evenly divided between vaccines administered simultaneously.
4. Pertussis and varicella disease risk figures have been adjusted up based on underreporting estimates.
5. Single vaccines are not available for diphtheria, tetanus or pertussis (DTP), or for measles, mumps or rubella (MMR).
6. Excluding the anomalous H1N1 pandemic year 2009.
The contents of this website are for informational purposes only. Opinions expressed should not be construed as medical advice.
The particulars of any person’s concerns and circumstances should be discussed with a qualified health care practitioner prior to making any decision which may affect the health and welfare of that person or anyone under his or her care.